| Definitions | Methodology | Data visualization | Classifications | Links | Contact |
Beginning of treatment within 24 hours from start of attack — start of attack, i.e., start of acute symptoms (in case of absence of acute symptoms unconsciousness). If nondescript or intermittent symptoms precede prolongated serious symptoms followed by emergency call, the start of attack is calculated from prolongated symptoms. If episodes with different symptoms took part, the start of attack should be calculated from episode with typical retrosternal chest pain lasting at least 20 minutes. If attack begins with nondescript slowly deepen symptoms (crescendo) the start of attack is not possible to specify. Treatment begins at the point of first medical contact.
Hospital admission — hospitalisation a patient in an inpatient facility in acute care (excl. nursing and rehabilitation care), involving a stay of at least 24 hours (admitted patient).
Hospitalised patient (attack) — for acute myocardial infarction (AMI) (ICD-10 dignosis codes I20 and I21) statistics each acute myocardial infarction is counted as one case (even if the patient has been treated with the same acute myocardial infarction in several hospitals). If the patient has recurrent acute myocardial infarction during the year, the corresponding number of cases has been considered.
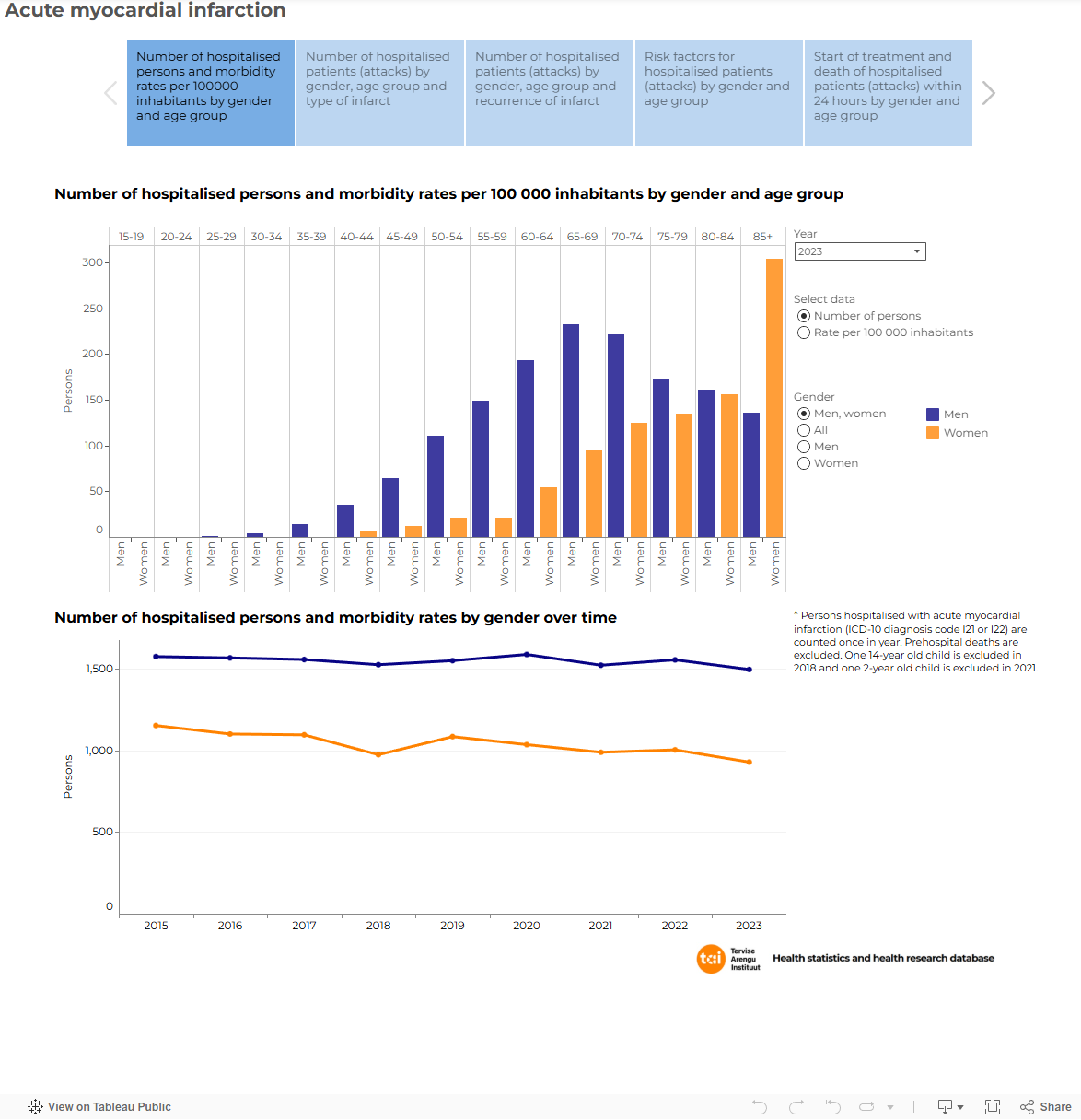
Hospitalised persons — persons who are Estonian residents and hospitalised with AMI (ICD-10 diagnosis code I21 or I22) are counted once per year. Person’s age is counted by last attack in case of recurrent AMI attacks during a year.
Mean annual population — half the sum number of the population at the beginning and at the end of the year.
Morbidity rate per 100 000 inhabitants — number of hospitalised persons with AMI (ICD-10 diagnosis code I21 or I22) is divided by the population. The mean annual population is used for calculation.
Number of persons with AMI — persons who are Estonian residents and hospitalised with AMI (ICD-10 diagnosis code I21 or I22) attack are counted once per year. Includes prehospital deaths. Person’s age is counted by last attack in case of recurrent AMI attacks during a year.
Risk factors:
Subtype of infarction:
The Estonian Myocardial Infarction Registry (EMIR) has been founded with the aim to improve the diagnosis and treatment of acute myocardial infarction and facilitate the planning of health care services for AMI as well as conduct epidemiological research.
EMIR is an electronic database including all hospitalised acute care cases of AMI (International Classification of Diseases 10th version codes I21.0–I21.9 and I22.0–I22.9) in Estonia about Estonian residents. Submitting data of patients hospitalised due to AMI is mandatory for all hospitals.
The use of the personal identification number (ID-code) enables linkage with other national registries (e.g., Population Register, Estonian Health Insurance Fund database and Estonian Causes of Death Registry).
For table "AMI01: Number of hospitalised persons with acute myocardial infarction and morbidity rates per 100 000 inhabitants by sex and age group" standardised rate European standard population (2013) is used.
Age distribution of European Standard Population, 2013
Total 100 000 0 1000 1–4 4000 5–9 5500 10–14 5500 15–19 5500 20–24 6000 25–29 6000 30–34 6500 35–39 7000 40–44 7000 45–49 7000 50–54 7000 55–59 6500 60–64 6000 65–69 5500 70–74 5000 75–79 4000 80–84 2500 ≥85 2500
The International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10)
This classification is used to code diagnoses and submit the data about disease cases in accordance with the diagnoses. The classification system is available on the webpage of the World Health Organization.
More detailed information in Estonian is available: https://www.kliinikum.ee/infarkt/
Gudrun Veldre
Estonian Myocardial Infarction Registry
Tartu University Hospital
Phone: +372 731 8459
E-mail: emir[at]infarkt.ee
Updated: 1.12.2025